
Coronary artery imaging is undergoing a revolution, thanks to multi-detector CT angiography (MDCTA). The best cardiac CT scanners now have excellent temporal and spatial resolution (83msec/0.6mm axial) and powerful analytical software that permit the most detailed non-invasive coronary artery imaging yet, including plaque visualisation, and the characterisation and quantitation of stenosis for both obstructive and non-obstructive plaque.
Powerful hardware and software now allow near-instantaneous multiplanar (MPR) imaging, enabling coronary artery imaging assessment through both space and time. Data is typically reconstructed into high-resolution 2D axial images, while MPR imaging yields images of non-ordinal structures, such as coronary arteries, walls, lumina and other complex cardiac anatomy. This is often achieved via automated centreline detection, easily permitting 3D assessment of the entire vessel.
Go deeper with GlobalData

Volume rendering techniques display cardiac anatomy as shaded surfaces, but due to resolution and image segmentation limitations, they currently have limited, although real, value (Figure 1). This value typically lies in visualising large anatomical structures (aneurysms, chambers and such) or the course of coronary arteries in cases of congenital anomalies or in chronic total occlusions (CTOs).
CORONARY DISEASE
Invasive coronary angiography typically visualises only the vessel lumen, but not the vessel wall or plaque. Sensitivity and specificity for disease detection in patient populations already selected for invasive coronary angiography are above 90%, and negative predictive values are 99%.
In an earlier study, we examined MDCTA in a clinical population of 994 consecutive patients. The accuracy of MDCTA in this setting was 87% by patient-based analysis and 89% by vessel-based analysis.
Non-obstructive and uncalcified plaque have a significant clinical impact. Plaque vulnerability may relate to remodelling and calcium patterns – a higher degree of remodelling and a ‘speckled’ pattern may be markers for vulnerability (Figure 2).
Uncalcified plaque may be the only manifestation of coronary artery disease in as many as 14% of patients, and appears to be associated with significant stenosis in only about 1% of cases with calcium scores of zero. Prominent risk factors include obesity and smoking. Since the majority of acute coronary syndromes are caused by plaque rupture or erosion of only moderately severe stenoses, plaque characterisation using MDCTA may provide a way of identifying these plaques.
The identification of plaques that have already undergone disruption has also been described. A retrospective analysis of 176 ambulatory patients who underwent MDCTA found 39 patients with high-density lesions (>130HU) within the extra-luminal space.
CLINICAL CARDIOLOGY
The superior spatial and temporal resolution of invasive angiography makes it the gold standard for stenosis detection and quantitation. However, MDCTA has excellent sensitivity and negative predictive value in most patient-based analyses compared with an invasive study, which is clinically important for evaluating atypical chest pain.
In a patient population with unclear stress test results, MDCTA showed excellent performance (sensitivity 98%) in effectively triaging these patients for coronary angiography. What is more, MDCTA costs roughly one third as much as coronary angiography.
MDCTA has a clear role as an adjunctive diagnostic test in patients at low to intermediate risk of coronary artery disease and an indeterminate cardiac stress test result.
An MDCTA that shows no significant stenosis (>50%) predicts an excellent short-term prognosis in this population (an event rate of 0.2% at six months). Coronary bypass grafts are well-visualised, due to their larger diameter and relative lack of motion.
MDCTA is increasingly being used in emergency departments (EDs). In the US alone there are more than one million ED visits each year for chest pain. Such visits are quite expensive – the charge for a single visit is typically $5,000–$15,000. In the US, the cost of emergency room (ER) chest pain visits may be between $10bn and $13bn a year.
Recent studies comparing nuclear and CT tests found that MDCTA is at least as accurate as nuclear stress imaging for the detection and exclusion of acute coronary syndromes in low-risk chest pain presenting to the ER. A subsequent study of ED chest pain patients found that MDCTA reduced patient time in the ED from 15 hours to 3.4 hours and cost about 20% less than standard chest pain evaluations. MDCTA had the additional side benefit of reducing the need for repeat evaluations over the long term, since the coronary disease status was known after the CT scan.
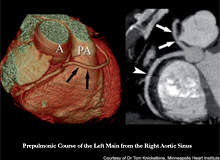
MDCTA is now the de facto standard for anomalous coronary arteries. Coronary artery anomalies are seen in 1% of all autopsies and approximately 0.5% of patients undergoing coronary arteriography. Most coronary artery anomalies are benign and remain clinically silent, allowing a patient a normal lifespan. However, if the anomalous coronary artery’s course runs between the aorta and the pulmonary artery or travels intramyocardially, an individual may be at risk of sudden death, myocardial ischemia or congestive heart failure.
Typically the evaluation of a young patient with syncope will not include coronary angiography, as the likelihood of obstructive coronary artery disease is low. However, 13% of young athletes who experience sudden death have anomalous coronary arteries. MDCTA not only shows the origin of the coronary artery, but it also delineates the course of the coronary artery in three dimensions as it relates to the great vessels and other cardiac structures.
FUTURE ROLE
As the temporal and spatial resolution of MDCTA continues to improve, applications for the technology are rapidly broadening. More accurate stenosis quantitation will be possible, and a strong alternative to invasive coronary angiography will emerge.
It will make possible the identification of non-obstructive plaque as either stable or vulnerable. This may permit prophylactic intervention based on plaque risk. MDCTA will also be able to identify asymptomatic patients with very early coronary artery disease who need aggressive preventative measures.
The role of CTA in the ED is developing, and it will probably reduce the cost of chest pain evaluation. CTA can also show important information about such structures as the left atrial appendage, documenting, for example, poor blood flow within this structure (Figure 3).
Cardiac CT is beginning to have a role in interventional procedures. The CTO remains a major interventional challenge. CT performed before intervening on the CTO can gather information on the plaque type (calcified, uncalcified), vessel curvature and lesion length, while new software is emerging that can assist in CTO intervention planning (Figure 4). CT is an excellent tool for selecting viewing angles for interventions, and is useful for creating an angiographic-equivalent image for use in
the cath lab to assist wire guidance and directional planning.
CT could be used in electrophysiology, to delineate anatomy prior to ablation or mapping, for example. Myocardial perfusion and viability imaging are likely to become a major application. CTA could also be useful for detecting left atrial appendage thrombus and patients at risk of atrial appendage emboli, due to poor blood flow into and out of the left atrial appendage. Detection, quantitation and follow-up of valvular lesions, including aortic stenosis and mitral valve disease is another promising area of MDCTA research.
Molecular imaging techniques are emerging for MDCTA. Clot visualisation by direct imaging of human plasma through anti-fibrin monoclonal antibodies is already being studied. This holds great promise for the early detection, localisation and characterisation of unstable plaque with developing thrombus. Monitoring gene and cell therapy is emerging as an interesting research application. There are few areas of cardiac physiology and anatomy that will not be affected and improved by cardiac CTA.
MDCTA technology is revolutionising cardiac imaging by enabling cardiac physicians to carry out detailed anatomical and physiological assessments of the heart. The key to further development will be obtaining images more rapidly and with higher spatial resolution. MDCTA is an inexpensive tool that can provide a broad range of valuable clinical information.
